AI Scribe: The Complete 2026 Guide To Reducing Documentation Burden & Scaling Your Practice

Introduction
For overwhelmed practice managers facing staffing shortages and mounting administrative burdens, the AI scribe represents a transformative solution that can scale operations without increasing headcount. In 2026, healthcare practices are increasingly turning to artificial intelligence to address provider burnout from excessive charting, reduce claim denials through improved documentation accuracy, and achieve the operational efficiency needed to remain financially viable. According to JAMA Network - Medical Research and Clinical Evidence, implementing AI-powered documentation systems can reduce provider documentation time by up to 70%, directly addressing the core challenges that keep practice managers awake at night. This comprehensive guide explores how AI scribe technology works, the specific benefits for practice operations, implementation considerations, and why unified agent approaches like HealOS deliver superior results compared to standalone solutions.
Understanding AI Scribe Technology in 2026
An AI scribe is an advanced healthcare automation tool that uses natural language processing, machine learning, and ambient voice recognition to automatically generate clinical documentation from patient-provider conversations. Unlike traditional medical transcription or human scribes, modern AI medical scribes operate in real-time during patient encounters, capturing nuanced clinical details while allowing providers to maintain eye contact and focus on patient care rather than computer screens.
How AI Scribe Technology Works
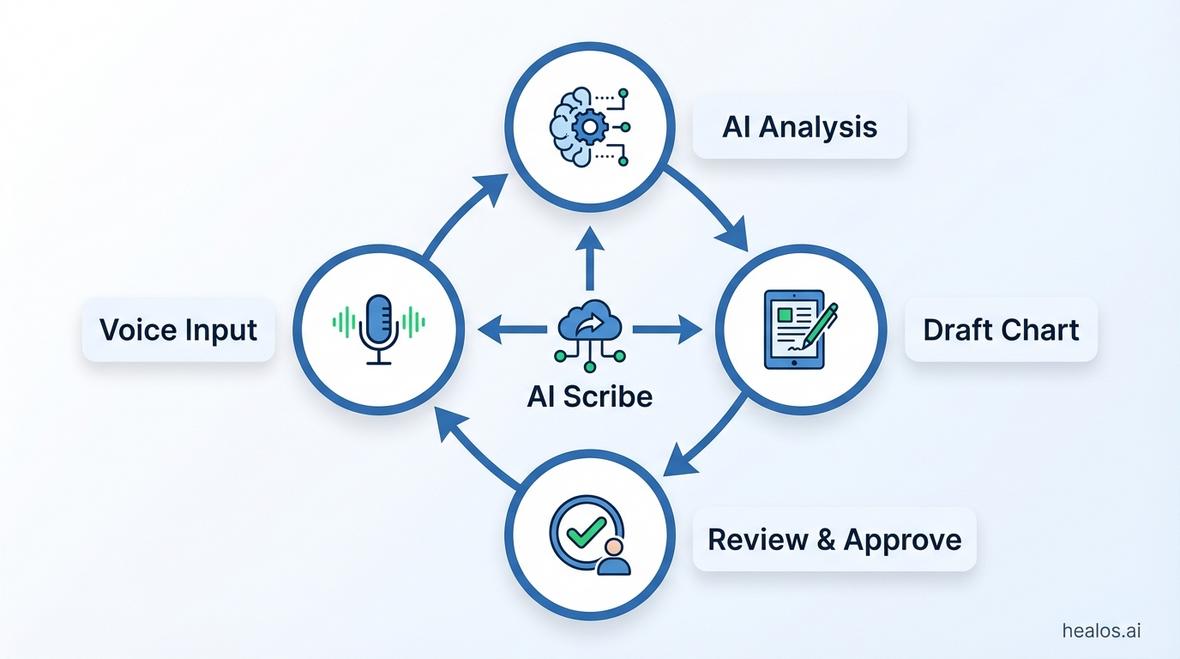
The AI scribe workflow follows a sophisticated four-step process that transforms spoken clinical encounters into structured documentation:
- Voice Input Capture: Advanced microphones and ambient listening technology capture the natural conversation between provider and patient without requiring specific dictation commands or rigid formatting
- AI Processing & Analysis: Machine learning algorithms trained on millions of clinical encounters parse the conversation, identifying relevant clinical information, distinguishing between patient history and provider assessment, and extracting key data points
- Draft Chart Generation: The system automatically generates structured clinical notes in formats like SOAP, DAP, or specialty-specific templates, populating relevant fields with appropriate clinical terminology and ICD-10 codes
- Provider Review & Approval: Clinicians review the AI-generated draft, make any necessary corrections or additions, and approve the final documentation for the medical record
This automated workflow typically reduces documentation time from 15-20 minutes per patient to just 2-3 minutes of review time, representing an 85-90% time savings that directly translates to operational capacity gains.
Ambient Clinical Intelligence vs. Traditional Dictation
The distinction between ambient AI scribes and older medical dictation software is critical for practice managers evaluating solutions. Traditional dictation requires providers to speak in structured formats, use specific commands, and often still requires manual typing for certain fields. Ambient clinical intelligence, by contrast, passively listens to natural conversations and automatically structures the information without provider intervention during the encounter. This fundamental difference explains why ambient AI scribes deliver substantially higher provider satisfaction and time savings compared to legacy dictation systems.
The Business Case for AI Scribe: What Practice Managers Need to Know
For practice managers focused on financial health and operational efficiency, the implementation of an AI scribe system delivers measurable returns across multiple dimensions that directly impact practice profitability and scalability.
Addressing Staffing Shortages Without Increasing Headcount
The healthcare staffing crisis continues to intensify in 2026, with practices struggling to find qualified clinical and administrative personnel. According to Statista Digital Health Market Analysis, small to medium practices implementing AI scribe technology reported the ability to see 25-35% more patients with existing provider capacity, effectively creating the equivalent of hiring additional providers without the $200,000+ annual cost per full-time physician.
Consider the mathematics for a three-provider primary care practice:
- Current capacity: 60 patients per day across three providers (20 each)
- Documentation time per patient: 18 minutes average
- Total daily documentation time: 18 hours (6 hours per provider)
- After AI scribe implementation: Documentation time drops to 3 minutes per patient
- Time reclaimed: 15 hours daily (5 hours per provider)
- New patient capacity: 78-80 patients per day (30% increase)
This capacity increase happens without hiring additional providers, expanding office space, or extending practice hours representing pure operational leverage that improves both revenue and provider work-life balance.
Reducing Claim Denials Through Documentation Accuracy
For practice managers responsible for financial health, claim denials represent one of the most significant revenue leakage points. Industry data shows that 5-10% of claims are initially denied, with documentation deficiencies accounting for approximately 35% of these denials. AI scribe systems address this problem through several mechanisms:
- Comprehensive capture: Ambient listening ensures all relevant clinical details are documented, reducing missing information denials
- Proper code assignment: AI systems trained on billing guidelines automatically suggest appropriate ICD-10 and CPT codes based on documented clinical findings
- Medical necessity documentation: Automated inclusion of clinical rationale that supports billed services and reduces medical necessity denials
- Consistency and completeness: Standardized documentation templates ensure all required elements are present for each encounter type
Practices implementing comprehensive revenue cycle management solutions that include AI scribe technology report 40-60% reductions in documentation-related denials, translating to 2-3% improvements in overall collection rates a substantial impact on practice profitability.
Combating Provider Burnout and Improving Retention
Provider burnout driven by administrative burden represents both a quality-of-care concern and a significant financial risk for practices facing turnover costs exceeding $250,000 per provider. The phenomenon of 'pajama time'—providers spending evenings and weekends completing documentation has become endemic in healthcare, with studies showing clinicians spend 1-2 hours on after-hours charting for every clinical hour worked.
AI scribe implementation directly addresses this burnout driver by eliminating the documentation backlog that forces providers into evening work sessions. Practices report that providers who previously spent 8-12 hours weekly on after-hours documentation can complete all charting during clinical hours after implementing AI scribe systems. This work-life balance improvement translates to measurable retention benefits and reduced turnover costs that significantly impact practice financial health.
Implementation Considerations for Practice Managers
Successfully deploying an AI scribe requires careful attention to several operational and technical factors that determine whether the implementation delivers expected returns or becomes another underutilized technology investment.
EHR Integration: The Make-or-Break Factor
The single most important technical consideration for AI scribe implementation is seamless EHR integration. Systems that require manual copy-paste workflows or separate documentation platforms fail to deliver the promised efficiency gains and typically see poor provider adoption. Practice managers should prioritize solutions offering:
- Direct EHR write-back: Documentation flows directly into the EHR without manual transfer steps
- Bi-directional data exchange: The AI scribe can pull patient context from the EHR and write completed notes back
- Native integration support: Pre-built connectors for major EHR platforms rather than generic APIs requiring custom development
- Single sign-on: Unified authentication that doesn't require providers to log into separate systems
HealOS distinguishes itself in this critical area through comprehensive EHR integration that works seamlessly with Epic, Cerner, Athenahealth, eClinicalWorks, and dozens of other platforms, ensuring the AI scribe becomes a natural extension of existing clinical workflows rather than a disruptive add-on.
Training Requirements and Change Management
Even the most sophisticated AI scribe technology delivers poor returns if providers don't adopt it effectively. Practice managers should budget for 2-4 weeks of transition time during which provider productivity may temporarily dip as clinical staff adjust to new workflows. Successful implementations typically include:
- Structured onboarding sessions: 1-2 hour training sessions that cover system operation, voice optimization, and review workflows
- Shadowing periods: Initial patient encounters where implementation specialists observe and provide real-time coaching
- Progressive rollout: Starting with early adopter providers before expanding to the full clinical team
- Ongoing optimization: Regular check-ins to refine custom templates and address emerging workflow questions
Practices should designate an internal 'AI scribe champion'—typically a tech-savvy provider or clinical leader who can troubleshoot common issues and encourage peer adoption during the transition period.
Privacy, Security, and Compliance Considerations
Practice managers bear ultimate responsibility for ensuring AI scribe implementations meet HIPAA requirements and protect patient confidentiality. Critical security considerations include:
- Data encryption: Both in-transit and at-rest encryption of all patient conversations and documentation
- Access controls: Role-based permissions ensuring only authorized personnel can access patient encounters
- Business Associate Agreements: Proper BAA execution with the AI scribe vendor establishing HIPAA compliance obligations
- Audit trails: Comprehensive logging of all system access and documentation modifications
- Data residency: Understanding where patient data is stored and processed, with preference for U.S.-based infrastructure
Reputable AI scribe vendors provide detailed security documentation, undergo regular third-party security audits, and maintain SOC 2 Type II certifications demonstrating robust security controls.
The Unified Agent Advantage: Why Standalone AI Scribes Fall Short
While many vendors offer standalone AI scribe solutions, practice managers seeking to truly scale operations without increasing headcount should understand the limitations of point solutions versus unified healthcare automation platforms.
The Problem with Point Solutions
Practices that implement standalone AI scribes often experience initial excitement followed by frustration when they realize documentation is only one piece of the administrative burden puzzle. Providers still face:
- Prior authorization delays: Time-consuming phone calls and fax exchanges for medication and procedure approvals
- Eligibility verification: Manual insurance verification processes that delay appointments and create billing issues
- Referral coordination: Administrative overhead managing specialty referrals and tracking patient follow-through
- Patient communication: Phone calls for appointment reminders, follow-up instructions, and routine questions
- Claims management: Denial follow-up, payment posting, and accounts receivable monitoring
Each of these functions requires separate staff time, and implementing a standalone AI scribe does nothing to address these ongoing operational challenges.
HealOS's Unified Agent Approach
HealOS differentiates itself through a comprehensive 'unified agent' platform that addresses the full spectrum of practice administrative workflows within a single integrated system. Practice managers implementing HealOS gain access to:
- AI Scribe: Ambient clinical documentation with specialty-specific templates and custom note formatting
- AI Receptionist: Automated phone answering, appointment scheduling, and patient intake that handles routine calls without staff intervention
- Prior Authorization Automation: Intelligent agents that submit, track, and follow up on prior authorization requests automatically
- Eligibility Verification: Automated insurance verification that runs before every appointment, eliminating surprise billing issues
- Referral Management: End-to-end referral tracking from initial order through specialist report receipt
- Revenue Cycle Management: Automated claims processing, denial management, and payment posting that reduces billing staff requirements
This unified approach means practice managers can address multiple operational bottlenecks simultaneously with a single vendor relationship, unified training, and integrated reporting rather than managing half a dozen point solutions with separate contracts, logins, and support channels.
Measuring AI Scribe ROI: Metrics That Matter for Practice Managers
Practice managers need concrete metrics to justify AI scribe investment and track whether implementations deliver promised returns. The most relevant KPIs fall into four categories:
Time and Productivity Metrics
- Documentation time per encounter: Track minutes spent on charting before and after implementation (target: 80%+ reduction)
- After-hours charting time: Monitor weekly hours providers spend on evening/weekend documentation (target: elimination of pajama time)
- Patients per provider per day: Measure capacity increases enabled by reclaimed time (target: 20-30% increase)
- Note completion lag time: Track time from encounter completion to note signature (target: same-day completion rate >95%)
Financial Performance Metrics
- Revenue per provider: Monitor changes in provider productivity translated to billing (target: 15-25% increase)
- Documentation-related denial rate: Track denials attributed to missing or inadequate documentation (target: 50%+ reduction)
- Collection rate: Overall percentage of billed charges collected (target: 2-3 percentage point improvement)
- Cost per encounter: Calculate total administrative cost per patient visit (target: 30-40% reduction)
Quality and Compliance Metrics
- Documentation completeness score: Audit notes for presence of required elements (target: >95% compliance)
- Coding accuracy: Measure alignment between documented services and billed codes (target: <3% error rate)
- Audit readiness: Percentage of notes that would withstand payer audit (target: >98%)
Provider and Staff Satisfaction Metrics
- Provider satisfaction scores: Survey clinicians on documentation burden and work-life balance (target: >80% satisfaction)
- Technology adoption rate: Track percentage of encounters using AI scribe (target: >90% after 60 days)
- Staff turnover rate: Monitor clinical and administrative staff retention (target: measurable reduction)
Specialty-Specific AI Scribe Considerations
While AI scribe technology delivers value across all specialties, practice managers should understand how documentation requirements vary and ensure their chosen solution addresses specialty-specific needs.
Primary Care and Family Medicine
Primary care practices benefit from AI scribe's ability to handle diverse encounter types from simple acute visits to complex chronic disease management within a single platform. Key requirements include robust progress note templates for ongoing conditions and support for preventive care documentation that satisfies quality reporting requirements.
Behavioral Health and Psychiatry
Mental health practices require specialized documentation formats like DAP notes, safety assessments, and treatment plan updates. Psychiatry-focused AI scribes should include psychiatric-specific terminology, medication management documentation, and appropriate handling of sensitive mental health information that may require additional privacy protections beyond standard HIPAA requirements.
Specialty Practices
Specialists in fields like cardiology, orthopedics, and oncology need AI scribes with specialty-specific templates, procedure note support, and integration with specialty-specific diagnostic systems. Practice managers should verify that their AI scribe vendor has experience in their particular specialty and can provide reference customers in similar practices.
Typical Implementation Timeline and Milestones
Practice managers should expect the following timeline for AI scribe implementation:
- Week 1: Planning and Preparation - Contract execution, technical requirements gathering, EHR integration setup, and identification of pilot providers
- Week 2-3: Initial Training and Pilot - Provider training sessions, initial patient encounters with implementation support, template customization based on pilot feedback
- Week 4-6: Optimization and Expansion - Refinement of custom templates, expansion to additional providers, troubleshooting workflow issues
- Week 7-8: Full Deployment - All providers actively using the system, staff training on support workflows, baseline metrics establishment
- Month 3+: Ongoing Optimization - Regular metrics review, continuous template improvement, expansion to additional modules if using unified platform
Practices using HealOS's comprehensive implementation support typically achieve full deployment faster than industry averages due to superior EHR integration and specialty-specific template libraries that minimize customization requirements.
Common Implementation Pitfalls and How to Avoid Them
Practice managers can learn from common AI scribe implementation mistakes:
- Insufficient provider buy-in: Involve clinical leadership in vendor selection and address skepticism through demonstration sessions with similar practices
- Inadequate training time: Don't rush implementation allow sufficient time for providers to become comfortable with the technology
- Poor integration planning: Verify EHR integration capabilities before contract execution, not after
- Unrealistic expectations: Understand that AI scribe improves efficiency but still requires provider review and approval
- Ignoring workflow redesign: Use AI scribe implementation as an opportunity to optimize entire clinical workflows, not just documentation
Future Trends in AI Scribe Technology
Practice managers planning for long-term operational strategy should understand emerging trends in AI scribe technology:
- Predictive clinical decision support: AI scribes that not only document but also suggest diagnostic considerations or treatment options based on presented symptoms
- Automated quality measure reporting: Direct extraction of quality metrics from clinical documentation for MIPS and value-based care reporting
- Patient-facing summaries: Automatic generation of patient-friendly visit summaries and after-visit instructions
- Multi-language support: Real-time translation for practices serving diverse patient populations
- Integration with remote monitoring: Incorporation of continuous monitoring data into clinical documentation for chronic disease management
AI Scribe vs. Alternatives: A Practice Manager's Comparison
Practice managers evaluating solutions should understand how AI scribes compare to alternatives:
AI Scribe vs. Human Medical Scribes
Human scribes cost $40,000-$60,000 annually per provider, require hiring and training, create scheduling dependencies, and introduce privacy concerns with additional personnel in exam rooms. AI scribes cost $200-$400 monthly per provider, work 24/7 without scheduling constraints, scale instantly, and eliminate privacy concerns from additional personnel. For detailed analysis, see our comparison of AI vs. human scribes.
AI Scribe vs. Traditional Medical Transcription
Traditional transcription requires providers to dictate notes after patient encounters, introduces 24-48 hour delays for note completion, costs $0.10-$0.20 per line, and provides no clinical intelligence or coding support. AI scribes work in real-time during encounters, enable same-day note completion, offer predictable monthly pricing, and include intelligent coding assistance.
Frequently Asked Questions About AI Scribe Implementation
How long does it take providers to become proficient with AI scribe technology?
Most providers achieve basic proficiency within 5-10 patient encounters and full comfort within 20-30 encounters, typically representing 1-2 weeks of clinical time. Practices should expect minor productivity dips during the first week followed by significant efficiency gains thereafter.
Can AI scribe technology work in noisy clinical environments?
Modern AI scribe systems use advanced noise cancellation and voice isolation technology that performs well in typical clinical settings. Extremely noisy environments (emergency departments, surgical suites with multiple people talking) may require targeted microphone placement, but standard outpatient exam rooms present no challenges.
What happens if the AI scribe makes an error in documentation?
AI scribe systems generate draft documentation that always requires provider review and approval before becoming part of the permanent medical record. Providers maintain complete control and responsibility for final documentation accuracy. Quality systems should include regular auditing to identify systematic errors that can be addressed through template refinement.
How does AI scribe technology handle different accents or speaking styles?
Leading AI scribe systems are trained on diverse voice samples representing various accents, speaking speeds, and communication styles. Most providers find that systems adapt to their individual speech patterns within the first few encounters, with accuracy improving over time as the AI learns individual provider tendencies.
Can practices use AI scribe for telemedicine visits?
Yes, AI scribe technology works seamlessly with telemedicine platforms, capturing virtual visit conversations just as effectively as in-person encounters. This capability proved particularly valuable during the telemedicine expansion driven by recent healthcare trends and remains relevant as hybrid care models become standard.
What patient consent is required for AI scribe usage?
Requirements vary by state, but best practice includes notification to patients that visits may be recorded for documentation purposes, typically through signage in exam rooms and language in general practice consent forms. Most patients readily accept this when informed that the technology allows their provider to focus more attention on them rather than a computer screen.
Conclusion
For overwhelmed practice managers facing staffing shortages, provider burnout, and mounting administrative costs, AI scribe technology represents a proven solution that delivers measurable returns across productivity, financial performance, and clinician satisfaction metrics. The key to maximizing value lies in selecting solutions that offer seamless EHR integration, comprehensive support, and ideally a unified agent approach that addresses the full spectrum of practice administrative workflows rather than documentation alone. HealOS stands out in the crowded AI scribe market by delivering not just ambient clinical documentation, but a complete automation platform that enables practices to scale operations without proportional increases in headcount. Practice managers ready to transform their operational efficiency should begin with a thorough assessment of current documentation workflows, clear definition of success metrics, and evaluation of vendors based on integration capabilities, specialty expertise, and comprehensive automation breadth. The practices thriving in 2026's challenging healthcare environment share a common characteristic: they've moved beyond manual administrative processes to embrace intelligent automation that amplifies human capability rather than replacing it.